First:Why do dentists recommend that you make full zirconia dentures?
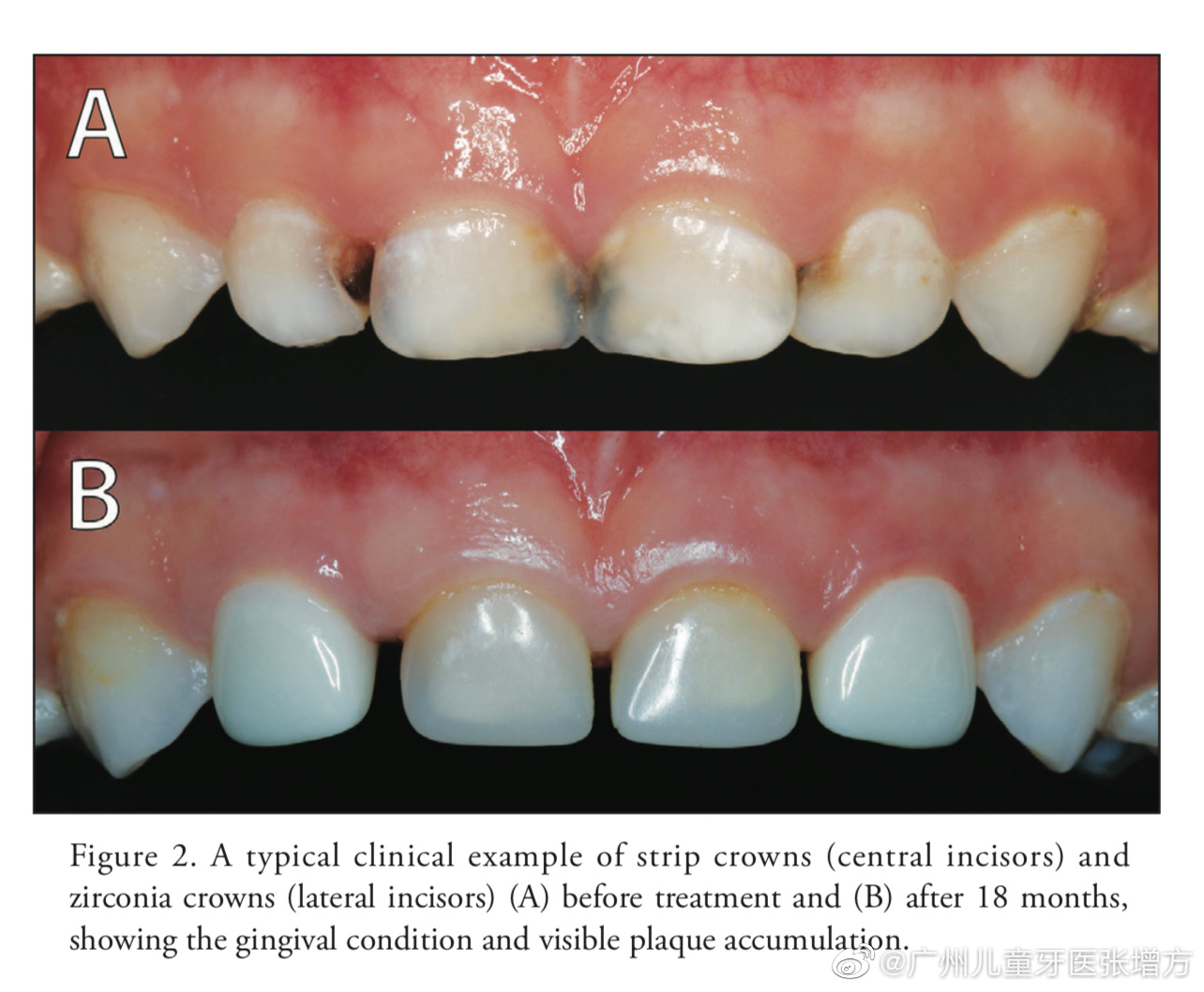
Having neat and beautiful teeth is one of the top ten health priorities for modern people, symbolizing status and representing a high-quality life. For a long time, zirconia dentures have been a fast and effective method for dental restoration. Unlike metal-based porcelain dentures, zirconia dentures do not have metal ions that can cause adverse reactions in the human body, such as black gums and gum atrophy. The absence of a metal inner crown allows for better translucence and color matching with natural teeth, eliminating the blue-gray effect that can occur under light. Additionally, zirconia materials are stable and less reactive to the acidic and alkaline environments found in the mouth. Patients also experience less interference from zirconia during CT and MRI scans. Hence, the dental community has been striving to promote metal-free zirconia options.

second:Is zirconia safe?
Zirconia materials used in dentistry have demonstrated excellent biological safety. Numerous experiments and clinical cases over the years have proven that zirconia is non-toxic and does not damage bone or soft tissue cells. No allergies have been reported.
Patients often worry about the radioactivity of zirconia. In fact, zirconia sourced from raw materials undergoes purification and processing steps, which remove all impurities. The State Administration of Food and Drug Administration has strict standards for all zirconia materials marketed as medical materials. Only after meeting these radioactive safety requirements can they be approved for clinical use. Furthermore, zirconia must meet the same radioactive qualification requirements as porcelain, alumina, and glass ceramics. Experiments have shown that pure zirconia powder is less radioactive than glass ceramics and even lower than human bone tissue.
Zirconia is sometimes mistakenly associated with metals. This confusion stems from a misunderstanding of chemical concepts. Zirconia is not a metal; while it may contain metal oxides, it is primarily a ceramic material. This is akin to the difference between sodium chloride (the chemical compound of salt) and sodium metal.
Third: is the failure rate of zirconia restorations high?
Research indicates that the rate of zirconia restoration failures is not higher than that of traditional porcelain restorations. Studies have found that zirconia failures primarily occur at the interface of the restoration rather than at the bond between the zirconia and the dental structure. The main reasons for these failures include:
Poor design of the underlying crown with overly thick local surfaces.
Improper temperature control during the zirconia sintering process, such as rapid cooling.
Inadequate post-treatment of the jaw adjustments, such as insufficient glazing or polishing.

4. Does the impact on the jaw affect zirconia restorations? How can it be avoided?
Jaw clenching can damage the surface of zirconia restorations, necessitating follow-up treatments like sintering or polishing. However, excessive grinding can significantly affect the strength of the restoration and may lead to fractures. If the production of the restoration is improper, it is advisable to use precision sealing. Minimal adjustments to zirconia can have a small impact on strength if adequate water cooling is applied. However, if the polishing area is too extensive, it will decrease strength. Communication with the technician is essential if adjustments to the inner crown are needed.
5. Will full zirconia cause excessive wear on the opposing teeth?
For patients with a tight bite and insufficient dental space, full zirconia restorations are a good choice. Concerns about excessive wear on opposing teeth are generally unfounded, as the abrasion resistance of zirconia depends on surface smoothness rather than hardness. Therefore, once polished or glazed, zirconia restorations will not cause excessive wear on opposing teeth.
6. What should I be aware of regarding zirconia adhesion? How does it differ from other full porcelain materials?
Zirconia bonding is relatively straightforward compared to glass ceramics due to its superior strength. There is no need for pre-treatment of the zirconia surface before bonding. The combination of active ions allows for a strong chemical bond. Various color options are also available.
Characteristics of zirconia:
Features:
Zirconia closely resembles the color of natural teeth, offering high aesthetic appeal and excellent light transmission. It is particularly suitable for high-quality dental restorations.
There is no metallic taste in the mouth, and zirconia does not corrode or irritate the pulp nerves due to temperature fluctuations. Its excellent biocompatibility ensures durability, enabling it to withstand high biting forces and prevent cracking. This effectively addresses issues associated with metal-based porcelain, such as discoloration and dark lines.
Indications:
Zirconia dentures are suitable for patients with aesthetic needs, severe tetracycline staining, fluorosis, deformities, or discoloration. Individuals with allergies to metal or plastic can still have front and rear crowns and bridges made of zirconia.
Zirconia crowns are also ideal for night guards, implant cases, and other scenarios prone to porcelain collapse.
Requirements for preparing the underlying teeth:
Anterior teeth: Reduce about 2.0 mm, with approximately 1.5 mm removed on the lingual side to prepare a 360-degree crown, about 1 mm wide, and an axial angle of 2 to 5 degrees.
Posterior teeth: Grind about 2.0 mm on the working side and 1.5 mm on the non-working side, with 1.5 mm reduction on both the buccal and lingual sides for a 360-degree preparation, about 1.0 mm wide, with an axial angle of 2 to 5 degrees.
Monolithic restorations: It is crucial to maintain a transitional step at the lingual edge, ensuring that this step does not interfere with the occlusal wear area. The surface reduction should be approximately 1.2 to 1.5 mm.
Precautions for clinical promotion of zirconia:
Short underlying teeth may be unsuitable for zirconia.
Insufficient space (weak connection points) may not be appropriate.
It is not advisable to use single inverted concave designs or inverted bridges.
Doctors should use silicone rubber for mold removal and 16 distinct color options to avoid color discrepancies.

Oral-Dr. Li
Delling Swan Pass Hospital




Leave a Reply