Unilateral free-end defects belong to the second category of the Kennedy Classification of Dental Defects, i.e., the defect in the arch is distal to one abutment tooth and may include other defects (subcategory). In this case, design considerations are focused on avoiding torsional damage to the adjacent gap abutments caused by “functional movement” of the denture. The type, number and layout of retainers, as well as the type and size of connectors, are based on the size of the gap and the health of the remaining teeth.
01 Maxillary unilateral free-end defect without subclass gap
I. Maxillary single posterior free end defects
1. Localized denture bracket design
( 1 ) The third molar is usually not restored.
( 2 ) Restoration of the second molar with partial denture to restore masticatory efficiency is limited, and the clinic is often used to control the overgrowth of the opposite teeth. The common single-ended movable bridge in China has a greater risk of accidental dislocation and swallowing, and cannot be used in the formal design of partial denture bracket. The first molar on the side of the gap can be designed – a group of three-armed card as a retainer, on the opposite side of the design of another group of three-armed card as an indirect retainer to the maxillary palatal bar connection.
2. Fixed denture restoration
( 1 ) Use single-ended bridge fixed denture to restore the second molar (to control the contact strength, mainly used to control the maxillary teeth overgrowth).
( 2 ) Restoration of second molars with implant denture (rarely used).
3. Decision not to restore
If the third molar does not exist, or if the second or third molar is missing, it is sometimes decided not to restore it after weighing the pros and cons (the risk of damage to the abutment teeth to restore masticatory efficiency).
The bracket of a removable partial denture restoring the second molar should provide reliable indirect retention in order to avoid the risk of accidental dislodgement of the denture during the exercise of its function and to provide protection for the abutment teeth adjacent to the gap. The classic design is to provide a set of clasps on the opposite side, which are attached to the gap side with a palatal bar. The disadvantage of this design is that it causes obvious foreign body sensation. If the conditions of the abutment teeth and alveolar ridge are good, an indirect retainer can be set in the ipsilateral first premolar, which causes less foreign body sensation, but the indirect retention is a little inferior, and at the same time, the possibility of exposing the metal color affecting the aesthetics is greater.
Unilateral free end defects of maxillary posterior teeth
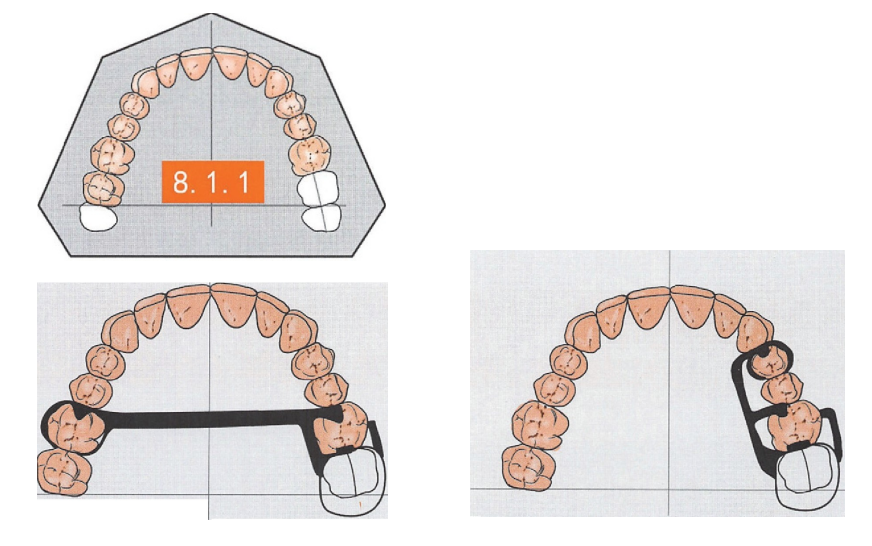
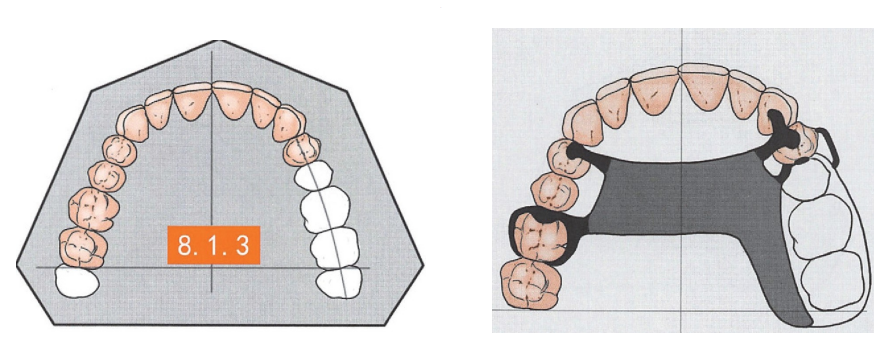
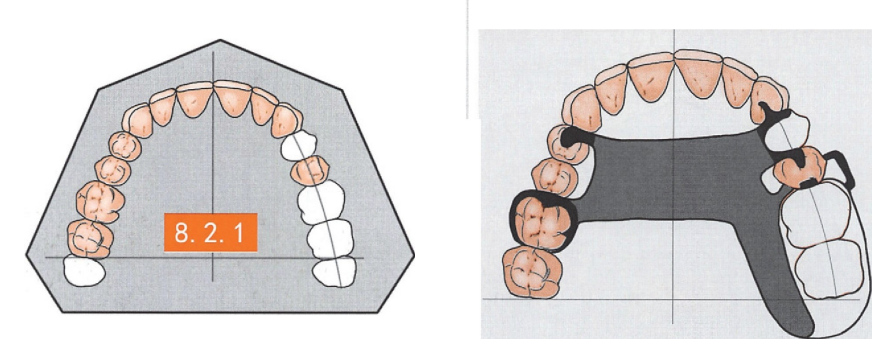
If the free-end defects of maxillary unilateral posterior teeth extend to the first molar, removable partial denture restoration is a common treatment option. The common features of bracket design are as follows.
1. The classic RPI ring set design is used on the abutment teeth adjacent to the gap to minimize the risk of torsional stress on the abutment teeth.
2. The guide surfaces are set distal to the adjacent gap abutments.
3. The contralateral side is used as an indirect retainer with the preferred abutment being a first molar with good support and retention profile.
4. Usually the maxillary palatal band connector is used, and the connector should avoid entering the anterior portion of the hard cheeks as much as possible in order to minimize the articulation obstruction and foreign body sensation.
5. If necessary, additional reserved brackets can be considered to provide further support and indirect retention.
The main focus of the design is to minimize the risk of torsional forces on the abutment teeth and to slow the process of alveolar ridge resorption. The attachment should avoid the lingual side of the abutment as much as possible to facilitate cleaning and maintain hard and soft tissue health. If the patient is sensitive to foreign objects on the hard palate and the abutment teeth are in good condition, the dentition support in the proximal mesial aspect of the first premolar can be eliminated and a narrower maxillary palatal bar connector can be used.
RP I ring set in Fig. 3. There are many variations in the position of the dentition support depending on the anatomical shape of the crowns of the abutment teeth, the occlusal relationship and the periodontal health condition.
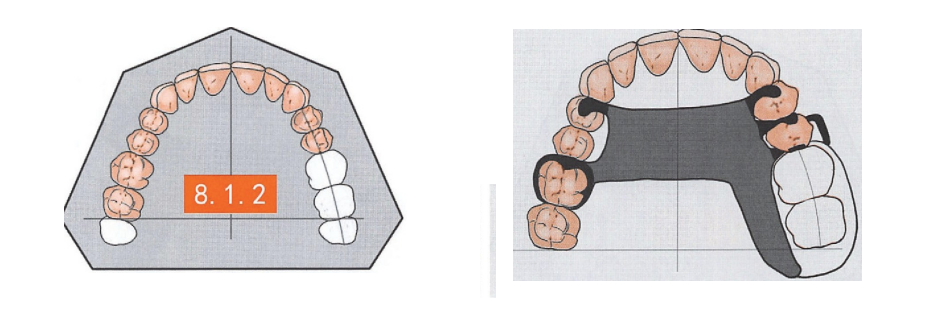
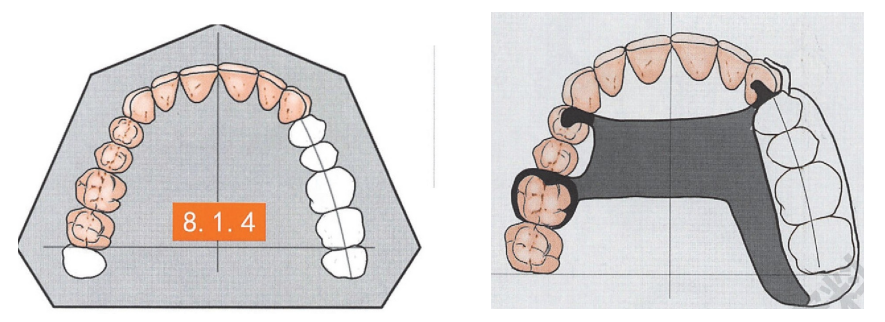
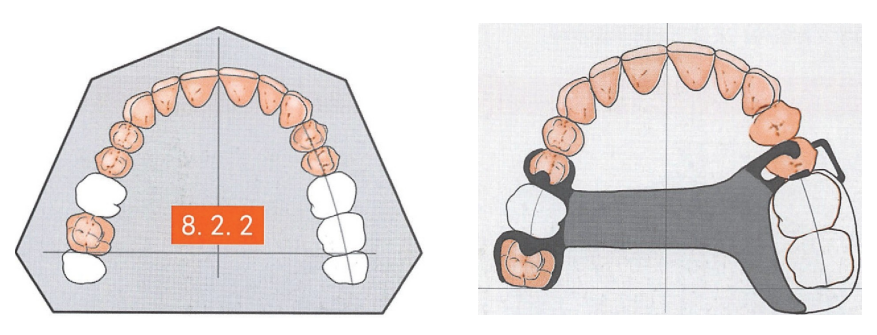
In the case of a unilateral loss of all molars and the second premolar, the design is based on Case 8.2.1, with the placement of an abutment in the lingual fossa of the cuspid on the side of the gap to provide additional support. Due to the increased size of the gap, it is necessary to place a dentition support on the contralateral first premolar and to use a larger maxillary palatal band connector.
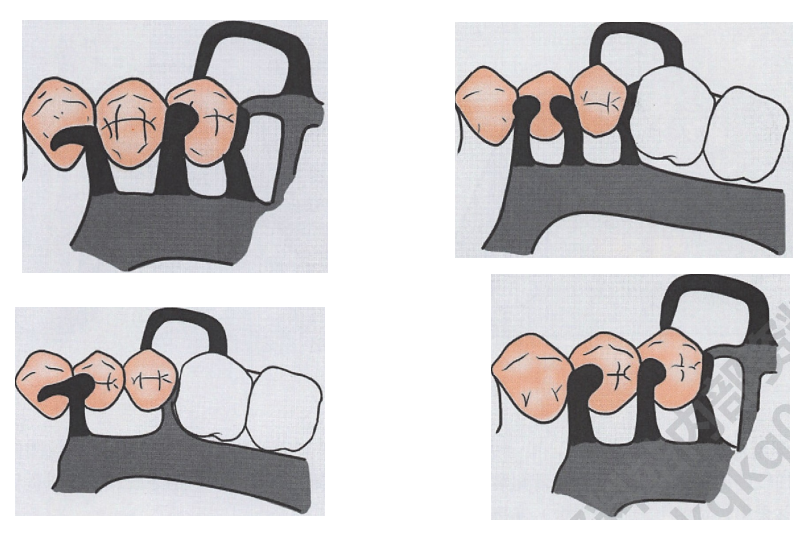
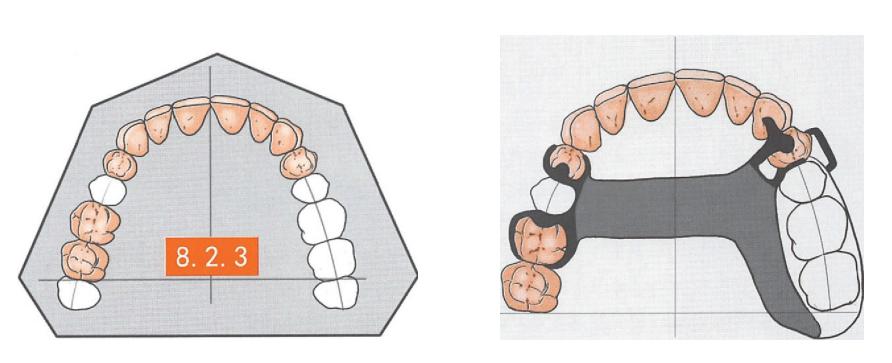
Unilateral loss of all molars and premolars, due to the anatomical limitations of the cuspids it is not possible to design an RPI ring set, on the gap side the cuspids are placed in the lingual fossa using a cold-formed ring with a more elastic steel wire, and the dentition support is placed in the lingual fossa. On the contralateral side an triennial support must be placed in the first premolar to provide indirect retention, and a wider maxillary palatal band (plate) connector is used.
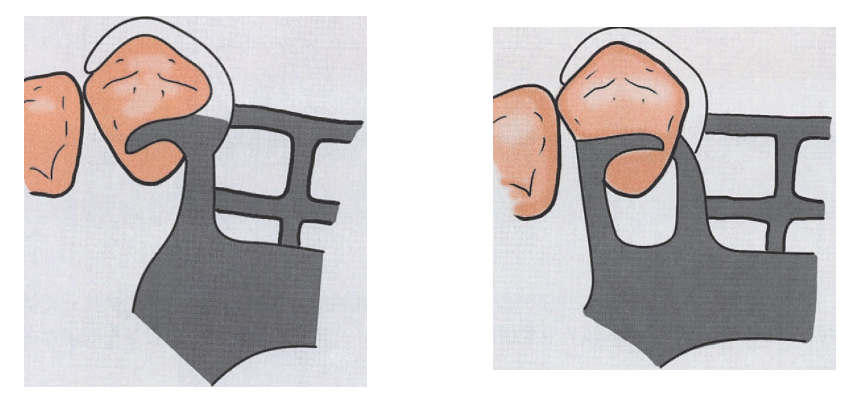
A wire cold-formed retainer is placed on the cuspids, and a lingual fossa is placed in the lingual fossa in a position determined by the anatomical shape of the lingual convexity, either proximo-central or disto-central.
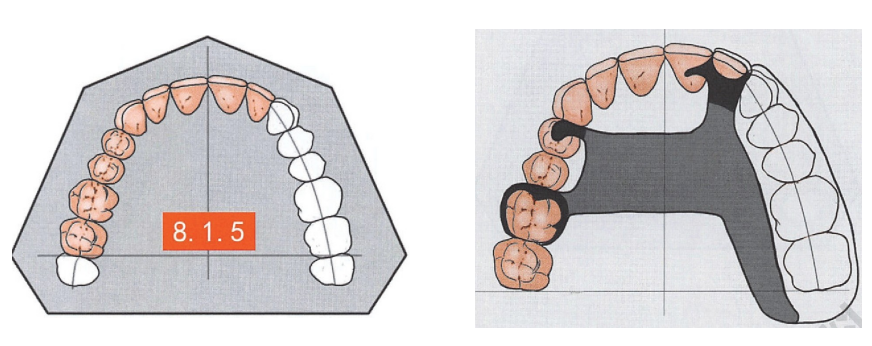
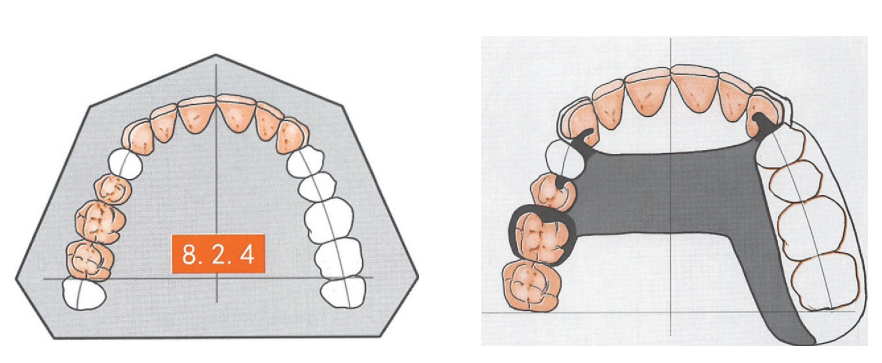
Unilateral loss of all molars, premolars and cuspids, due to the anatomical limitations of the lateral incisors, it is not possible to place the dental support in the lingual fossa, and a cold-bent ring with good elasticity is used, and the dental support is placed in the lingual fossa of the neighboring mesial incisors. A maxillary palatal plate connector was used and the extension was extended accordingly.
02 Maxillary unilateral free-end defects involving posterior subclass defects
I. Maxillary unilateral free-end defects involving ipsilateral subclass gaps
Common features of bracket design
If a maxillary unilateral free-end defect involves an ipsilateral additional posterior nonfree gap, it belongs to the subclass II of Kenne dy’s Classification of Dental Defects. The bracket design concept is not much different from that of the absence of a subclass gap, with attention paid to the position of the guide surfaces and the dentition support to maximize the use of the gap that exists.
An additional non-free gap in the first premolar on the same side as the free end gap is augmented with support by placing an interdental support in the lingual fossa of the cusp adjacent to the gap. A set of three-armed cards is used as indirect retention on the contralateral side, and additional dentition support brackets on the first premolar may be considered to further improve indirect retention. A maxillary palatal band connector is used.
II. Unilateral free-end defects of the maxilla involving a contralateral subclass of gap
Common features of bracket design
If a maxillary unilateral posterior free-end defect involves an additional contralateral posterior non-free gap, it belongs to subclass II of the Kennedy Classification of Dental Defects. The common features of bracket design are as follows.
1. The more protective RPI retainer set design should still be used as much as possible in the adjacent free-end gap abutment.
2. The guide surfaces are set in the distal and distal C of the adjacent gap abutments and the proximal and distal C of the adjacent subclass II gap abutments.
3. The first molar with good support and retention profile should be preferred for the abutment with indirect retention, and the existing gap space should be utilized as much as possible to provide indirect retention bilaterally to each other.
4. In order to minimize articulation obstruction and foreign body sensation, the connectors should avoid entering the anterior part of the hard palate as much as possible.
There is an additional non-free first molar gap on the opposite side of the free end of the gap, which is utilized to set up two sets of three-armed clips, and the width of the maxillary palatal band connector can be appropriately reduced by paying attention to the formation of adequate tooth support conditions during the preparation of the alveolar support sockets.
Compared to Case 8.2.2, the free end gap is enlarged and the contralateral non-free gap is shifted towards the proximal center. An amalgam bracket was placed in the lingual fossa of the cuspid on the side of the free end gap to enhance support. Two sets of three-arm clips are placed in the contralateral non-free space, and care is taken to create adequate tooth support during preparation of the sockets. A maxillary palatal band connector is used.
Compared to Case 8.2.3, the free end gap is further enlarged and the contralateral non-free gap is shifted towards the proximal center.
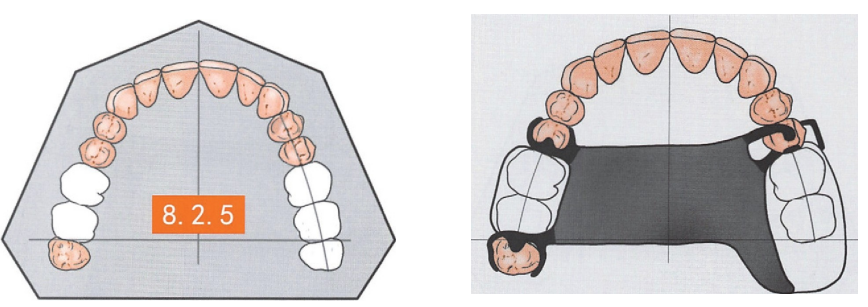
Compared to Case 8.2.2, the contralateral non-free gap involves two molars, but the third molar is present and can serve as an abutment. Two sets of three-armed clasps are placed in the contralateral non-free space (sometimes cast or cold-formed wire clasps may be considered for the third molar due to the high degree of variability in anatomical shape and longitudinal inclination of the teeth), and care is taken to create adequate tooth support during preparation of the alveolar support sockets. The connectors are made of wide maxillary cheek plates (sometimes a separate anterior-posterior palatal band can be considered depending on the situation).
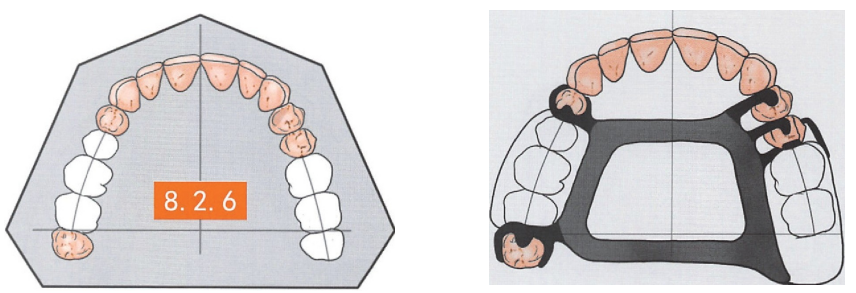
In contrast to Case 8.2.5, the contralateral non-free space is enlarged to include two molars and a premolar, but the third molar is present and can serve as an abutment. An RPI ring set was used on the abutment teeth of the adjacent free end gap and a proximal mesial support was added to the first premolar. Two sets of three-armed clasps were set up in the contralateral non-free space, and care was taken to create adequate tooth support conditions during the preparation of the triennial support socket. Separate anterior-posterior palatal band connectors are used to increase stability and reduce foreign body sensation.
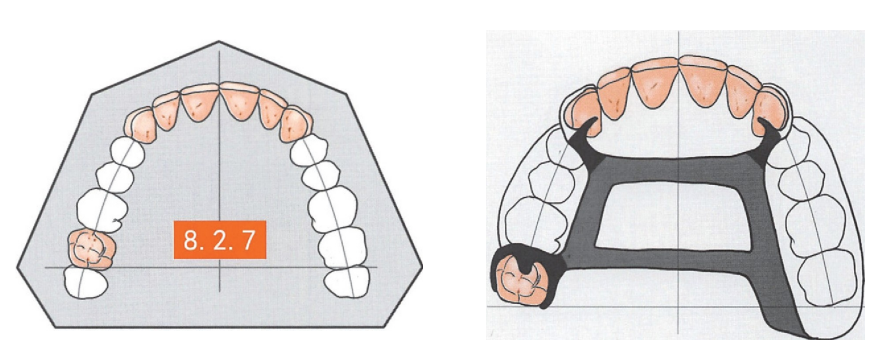
Compared to Case 8.2.6, the free space was enlarged to include all posterior teeth and the contralateral non-free space was moved forward to include the first molar and both premolars. The corresponding design used a more resilient wire cold-formed ferrule in the adjacent free end gap abutment (cusp) and placed a dentition support in the lingual fossa. In the contralateral non-free gap, the cuspids on the proximal mesial side were prepared with wire cold-formed rings and denture supports were placed in the lingual sockets. On the distal mesial side, the second molar is prepared in a socket to form a set of three-armed clasps. Separate anterior-posterior palatal band connectors are used.
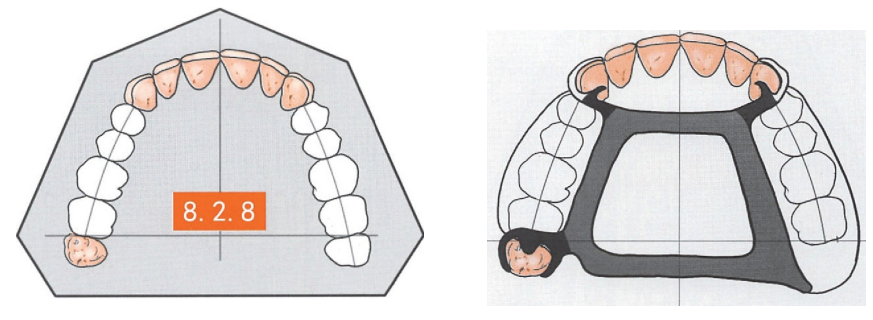
In contrast to Case 8.2.7, the contralateral non-free space is enlarged to include two molars and two premolars, but the third molar is present and can serve as an abutment. The wire cold-formed ring/lingual fossa support combination was still used on the bilateral cuspids. On the non-free gap side, the third molar is prepared for the dentoalveolar socket and a set of well-supported three-armed clasps or loop clasps are designed to support the retention. Separate anterior-posterior palatal band connectors are used.
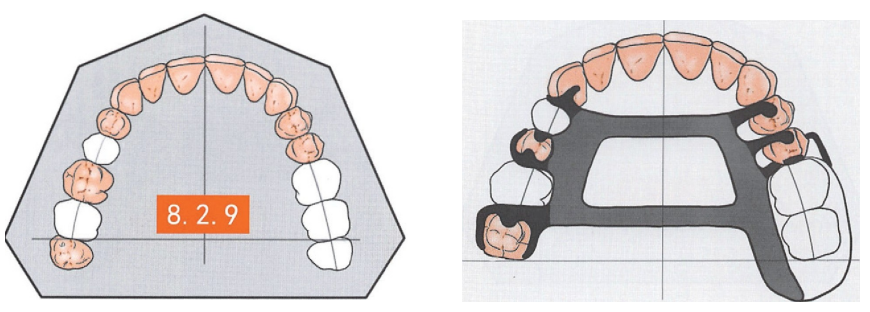
In contrast to Case 8.2.6, the contralateral side has two spaced non-free gaps. Three dentition support brackets are placed on this side to create adequate tooth support. Groups of three-armed cards were formed on each of the first premolar and second molar. Separate anterior-posterior palatal band connectors are used .
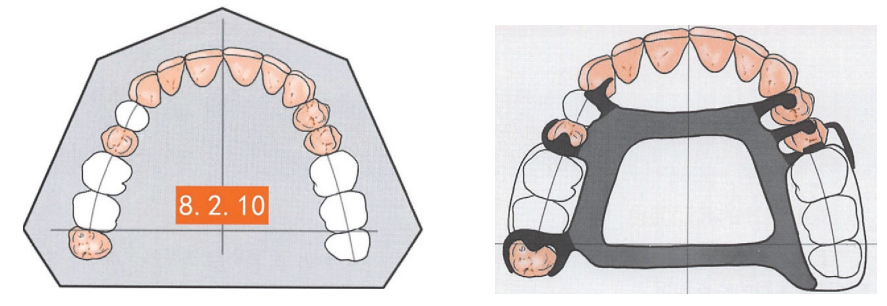
In contrast to Case 8.2.9, the non-free gap in the contralateral distal mesial extends to include both molars, but the third molar is present and can serve as an abutment. Three dentition support brackets were placed in the contralateral non-free gap to create adequate tooth support. Three sets of three-armed clasps are formed on each of the first premolar and the third molar (the third molar may be considered as a ring clasp depending on the situation). Separate anterior-posterior palatal bands are used.
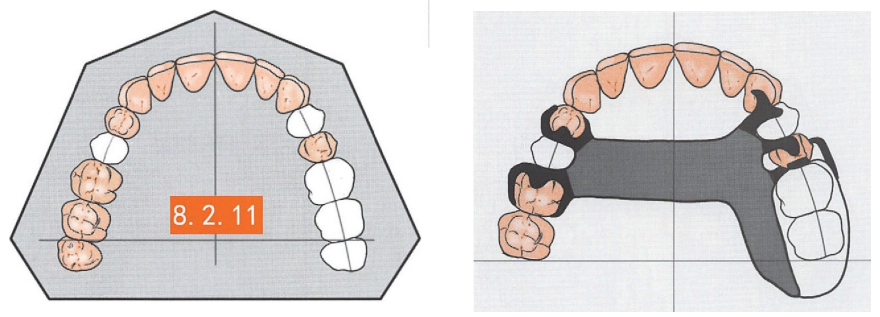
Referring to Case 8.2.1, a gap is created in the contralateral second premolar. The abutment teeth adjacent to the free gap remain in the RPI ring set. Dental brackets were placed in the lingual sockets of the cusps adjacent to the additional gap for additional support. A set of three-armed clips were used as retainers in the contralateral gap proximally and distally, using maxillary palatal band connectors.
03 Maxillary unilateral free-end defects involving anterior subclass defects
I. Unilateral free end defects in which the subclass gap is confined to the anterior region
Unilateral free-end defects of the maxillary posterior teeth involving an anterior gap also belong to subclass II of the Kennedy Classification of Dental Defects. The common features of bracket design are as follows.
1. The abutment teeth adjacent to the free end gap should still be designed with a protective RPI ring set as much as possible.
2. The guide surfaces are set in the distal and distal parts of the adjacent gap abutments and in the proximal and distal parts of the adjacent subcategory of gap abutments.
3. The abutment for indirect retention is preferred to the contralateral first molar to maximize the use of the gap space available.
4. The attachment will inevitably enter the anterior part of the hard palate, but the lingual side of the natural teeth should be avoided as much as possible in order to maintain good health.
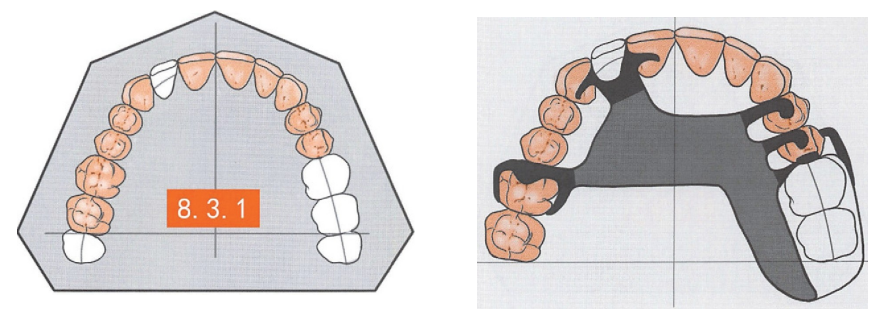
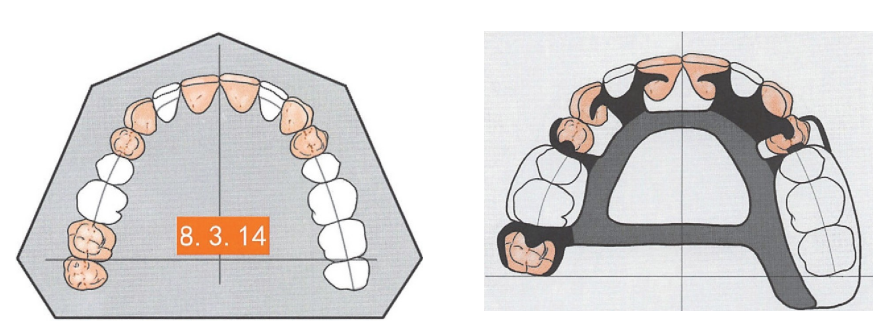
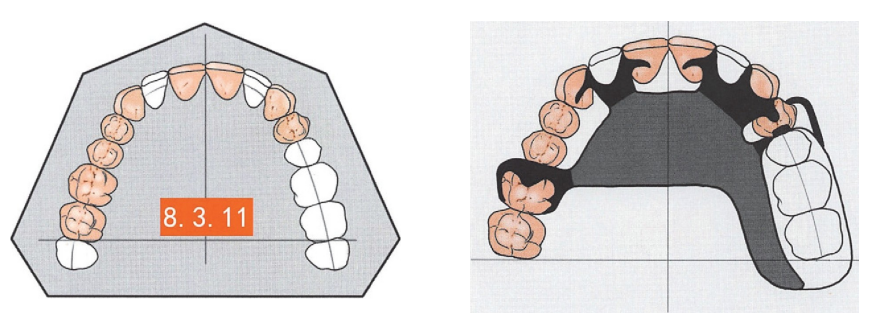
All molars are missing on one side, and a subclass of gap is present in the contralateral lateral incisor. The bracket design is based on Case 8.2.1 and is augmented, if possible, by the placement of dentition brackets in the lingual sockets of the mesial incisors and cuspids adjacent to the subclass gap. On the contralateral side, a set of three-armed clips is used as indirect retention, with a maxillary palatal plate connector, to avoid contact with the remaining teeth lingually as far as possible to allow for cleaning and self-cleaning space.
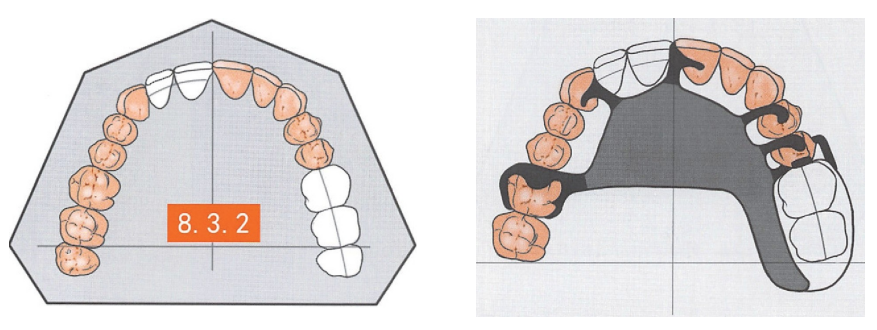
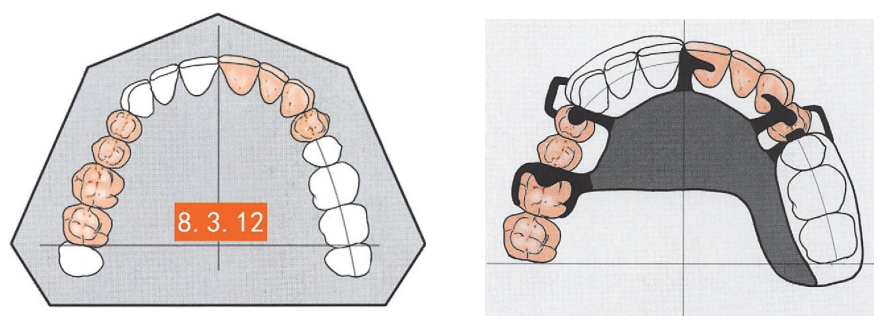
All molar teeth on one side are missing, and the subclass gap includes the contralateral mesial and lateral incisors. The bracket design is based on Case 8.3.1, with the maxillary palatal plate connector avoiding complete coverage of the anterior hard palate when possible.
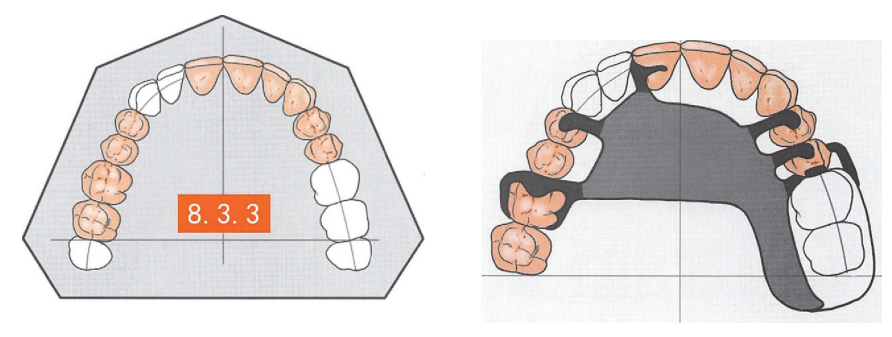
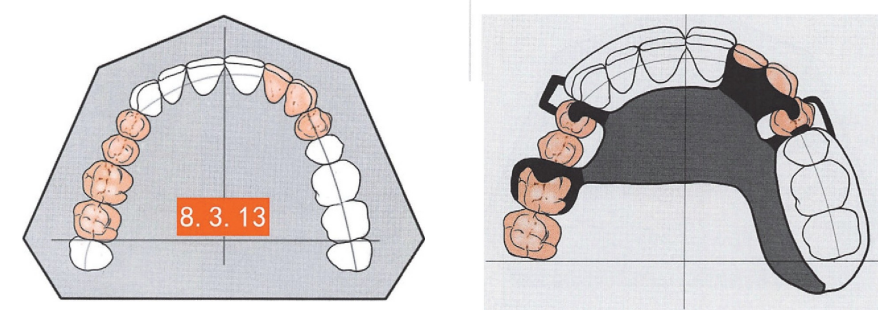
The design of the brace is along the lines of Case 8.3.1 and Case 8.3.2.
One side is missing all the molars, and the subclass of defects consists of mesial incisors bilaterally and lateral incisors contralaterally. The design of the bracket is characterized by the placement of dentition supports on the well-developed lingual convexity of the cuspids bilaterally, with the maxillary palatal plate connector covering the anterior hard palate, but trying to avoid complete coverage of the lingual side of the remaining natural teeth.
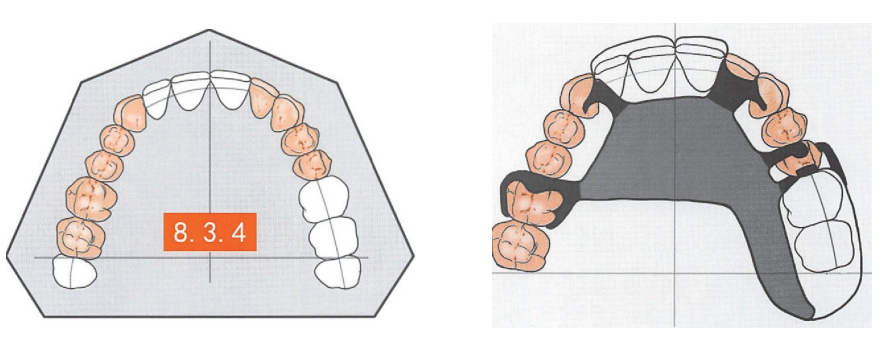
One side of the mouth is missing all the molars, and the subclass of defects consists of the mesial and lateral incisors bilaterally. The bracket design is characterized by a dentition support on the well-developed lingual ramus of the bilateral cusps, and the maxillary palatal plate connector covers the anterior portion of the hard palate, but still tries to avoid complete coverage of the lingual side of the remaining natural teeth.
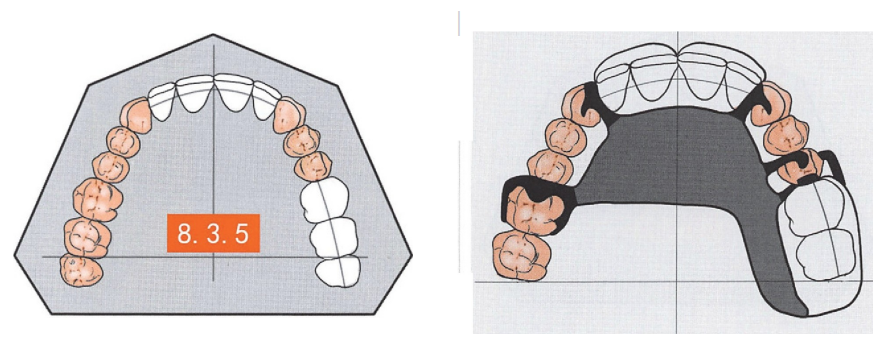
All the molars were missing on one side, and the two subclasses of gaps included the lateral incisors on the same side and the mesial and lateral incisors on the opposite side. The bracket design is characterized by a dentition support on the well-developed lingual convexity of the bilateral cusps and a maxillary palatal plate connector covering the anterior part of the hard palate, but still trying to avoid completely covering the lingual side of the remaining natural teeth.
All the molars on one side as well as the second premolar were missing, and the subclass of gaps included bilateral mesial incisors, lateral incisors, and contralateral cuspids. Since the inverted recesses of the first premolar tended to be concentrated in the proximal mesial, and considering the risk of a longer anterior gap forming a lever force arm, instead of designing a conventional three-armed card in the first premolar on the contralateral side, a combination of proximally mesial dentition brackets with an I-bar was used as a retainer to minimize torque on the abutment teeth. At the same time, a set of three-armed cards was designed as indirect retention in the first molar on that side, and lifting brackets were placed lingually on the ipsilateral cuspids to enhance support and stabilization, with the maxillary palatal plate as the large connector.

All molar teeth on one side and the second premolar are missing, with a subclass of gap in the ipsilateral mesial incisor. The bracket design is based on Case 8.2.2, with lifting brackets placed in the lingual sockets of the cuspids on the side of the gap for additional support, if possible. If the lingual sockets of the incisors adjacent to the anterior gap are well developed, a syndesmotic brace may be placed to enhance support and stability. A set of three-armed cards is used as indirect retention on the contralateral side, and additional dentition support brackets on the first premolar are often considered to provide further indirect retention, using a maxillary palatal plate connector .
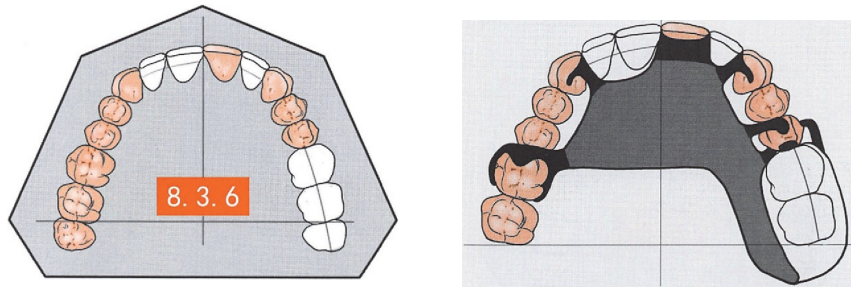
All of the molars on one side as well as the second premolar are missing, with a subclass of gap present in the contralateral cuspids . Dental support brackets were placed in the proximal mesial and (when possible) lingual fossae of the contralateral first premolar to enhance support. Indirect retention was reinforced with a set of three-armed clips in the first molar, using a maxillary palatal plate connector.
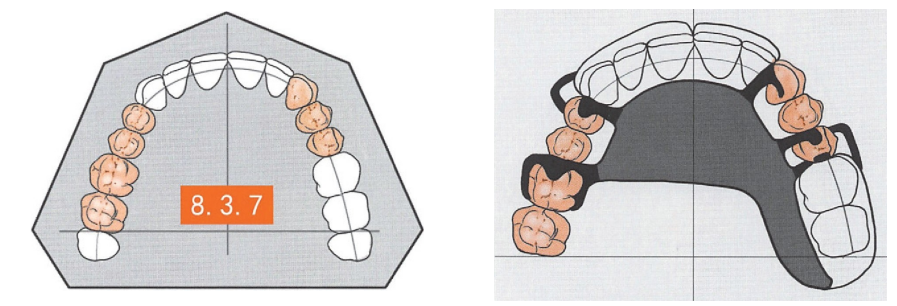
All the molars on one side as well as the second premolar were missing, and the subclass gap included bilateral mesial incisors. To simplify the structure, a maxillary palatal plate connector is used to cover the anterior portion, but every effort is made to avoid completely covering the lingual side of the remaining natural teeth.
All the molars on one side as well as the second premolar are missing, and the subclass of defects includes the lateral incisors bilaterally. The placement of dentition supports on the lingual side of the mesial incisors and cuspids facilitates supportive stabilization, and the maxillary palatal plate connector in the overlying anterior portion should be avoided as much as possible to completely cover the lingual side of the remaining natural teeth.
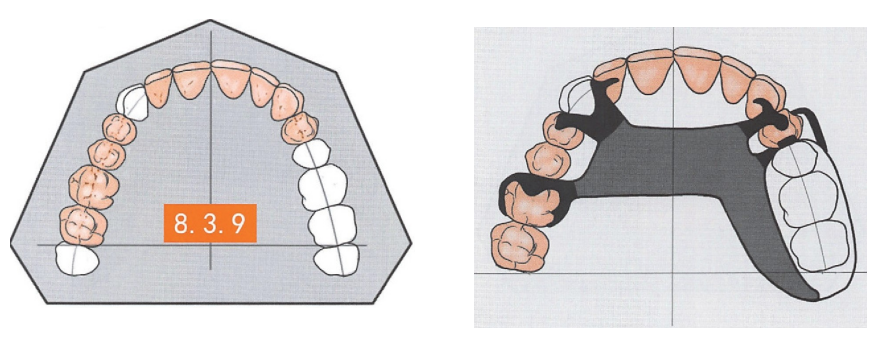
All the molars on one side and the second premolar are missing, and the subclass of defects includes the contralateral mesial incisors, lateral incisors, and cuspids. The design concept is based on Case 8.3.7, where the mesial incisors and cuspids are supported and stabilized by lingual placement of dentition brackets, and the maxillary palatal plate is used as a large connector.
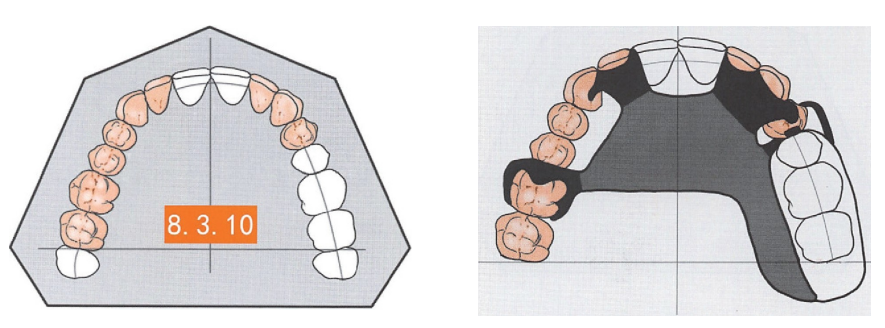
All the molars on one side as well as the second premolar are missing, and the subclass of defects includes bilateral mesial incisors, contralateral lateral incisors and cuspids. A similar design scheme was utilized for the same reasons as in Case 8.4.13.
Second, the subclass of defects involves unilateral free-end defects in the anterior and posterior regions of the teeth
The unilateral free-end defect of the maxillary posterior teeth involves separate anterior and posterior gaps and also belongs to the subclass of Kennedy’s Classification of Dental Defects. The common features of bracket design are as follows.
1. A more protective RPI ring set design should still be used for adjacent free-end gap abutments as much as possible.
2. The guide surfaces are set in the distal and distal parts of the adjacent gap abutments and in the proximal and distal parts of the adjacent subclass of gap abutments to ensure a smooth common seating path.
3. The abutment teeth for indirect retention are preferred to the contralateral first molar to maximize the use of the available gap space and to provide indirect retention to each other bilaterally.
4. The attachment will inevitably enter the anterior part of the hard palate, but the lingual side of the natural teeth should be avoided as much as possible in order to maintain good health.
All the molars on one side are missing as well as the second premolar, and the three subclasses of defects include the lateral incisors bilaterally and the second premolar and first molar on the opposite side. A set of three-arm cards at each end of the contralateral nonfree gap is the classic design. The placement of triennial brackets on the lingual side of the mesial incisors and cuspids facilitates enhanced support and stabilization, and an anterior-posterior palatal band connector is used in order to reduce the coverage area.




Leave a Reply