
The pontic is the part of the fixed dental prosthesis that restores the shape and function of the missing tooth. An ideal pontic should meet the following requirements: restore the shape and function of the missing tooth; be aesthetically pleasing and comfortable; possess good chemical stability; have effective self-cleaning properties; not irritate the remaining alveolar ridge and mucosa; and have good mechanical strength to withstand occlusal forces.
The design of the pontic’s morphology is divided into three parts: the design of the occlusal surface, the gingival surface, and the axial surface.
I. Design of the Occlusal Surface of the Pontic
The design of the occlusal surface of the pontic should consider the overall shape, size, and location of contact points.
1. **Overall Shape**
The occlusal surface morphology should be restored based on the anatomical form of the missing tooth and the occlusal relationship with adjacent teeth. On this basis, the height of non-functional cusps should be appropriately reduced to minimize the torque on the fixed bridge.
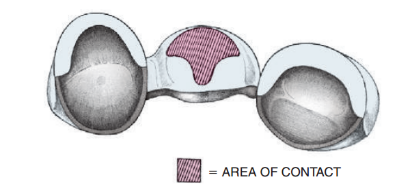
2. **Location of Contact Points**
Occlusal contact points should be evenly distributed, as close as possible to the centerline of the occlusal surface of the abutment teeth.
3. **Surface Area**
To reduce occlusal force and lighten the load on the abutment teeth, the occlusal surface area of the pontic should be minimized. This can be achieved by increasing the buccolingual gap between the pontic and the retention structure, enhancing food escape pathways, and reducing the cusp slopes on the occlusal surface.
By reducing the buccolingual diameter of the pontic, the occlusal surface area can be minimized. The following principles should be followed:
– The buccolingual diameter of the pontic’s occlusal surface should generally be 2/3 of the width of the missing tooth; in cases where the abutment conditions are poor, it can be reduced to 1/2 of the missing tooth’s width.
– If both abutment teeth are in good condition, restoring a single missing tooth can recover about 90% of the occlusal surface area; for two missing teeth, about 75%; and for three consecutive missing teeth, about 50%.
– In unilateral fixed bridges, due to the leverage effect, reducing the occlusal surface area is even more necessary, with a reduction of 1/3 to 1/2 in the buccolingual direction. For a unilateral bridge restoring a distal free-end edentulous area, the mesiodistal diameter can also be reduced by 1/3 to 1/2.
When designing clinically, it is essential to flexibly apply considerations based on the patient’s age, location of edentulous areas, and occlusal relationships. Additionally, it is important to note that reducing the occlusal surface area may increase the number of chewing cycles and prolong the total chewing time.
II. Design of the Gingival Surface of the Pontic
The gingival surface of the pontic can be designed in various forms, each with its own advantages and disadvantages, which should be selected based on clinical conditions.
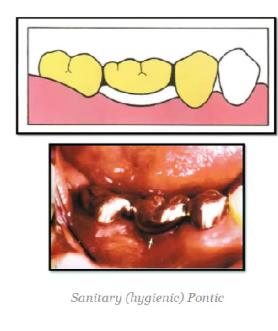
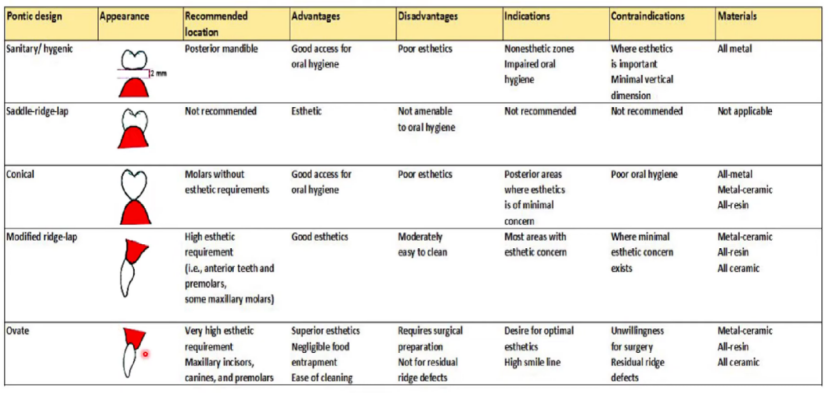
1. **Hygienic Pontic / Suspended Pontic**
The hygienic pontic has a 2-3 mm gap between itself and the alveolar ridge, making it easy to clean and preventing food impaction. However, it may be aesthetically unpleasing and can affect phonetics, so it is mainly used in non-aesthetic areas such as the posterior mandible. It is important that there is sufficient vertical distance in the edentulous area to accommodate this additional 2-3 mm; otherwise, the height of the pontic will need to be reduced, increasing the risk of fracture. Additionally, the gingival surface of the hygienic pontic can be modified to be arch-shaped for improved strength.

2. **Conical Pontic**
Similar to the hygienic pontic, the conical pontic also facilitates cleaning. However, its contact with the alveolar ridge is point contact, providing better aesthetics compared to the hygienic pontic. It is suitable for posterior areas but not for wide alveolar ridges, as the narrow pontic gingival surface may lead to food impaction. Furthermore, the curvature of the conical gingival surface should be adapted to the width of the alveolar ridge.
3. **Saddle Pontic**
The gingival surface of the saddle pontic resembles a saddle, providing extensive contact with the mucosa, thus achieving a better aesthetic effect. However, this design makes it difficult for patients to use dental floss to clean the concave gingival surface, which can easily lead to mucosal inflammation. It is generally used only for temporary restorations.

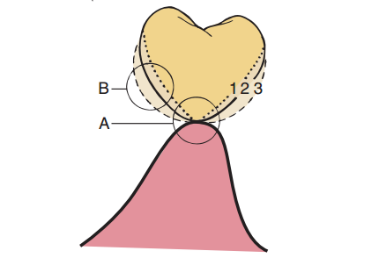
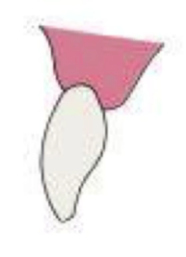
4. **Crest-Form / Modified Crest-Form Pontic**
The crest-form pontic, also known as a lateral pontic, has a triangular opening on the lingual side compared to the fully covered buccolingual side of the saddle pontic. Its gingival surface contacts the mucosa linearly on the labio-buccal side. It is easier to clean than the saddle pontic but may still allow food retention in the lingual gaps. The modified crest-form pontic expands the contact area on the labio-buccal side to the top of the alveolar ridge, creating a T-shaped contact surface. The modified crest-form pontic combines the best features of hygienic and saddle pontic designs, balancing aesthetics and ease of cleaning, and is suitable for aesthetic areas such as anterior teeth.


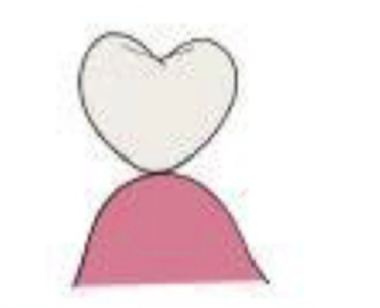
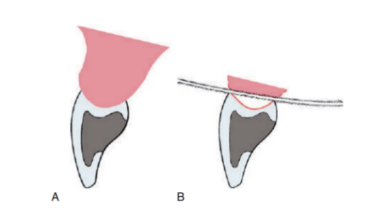
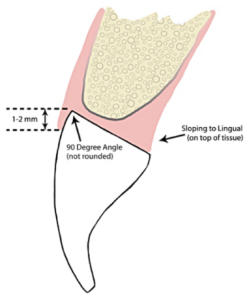
5. **Oval Pontic**
The oval gingival surface design is the most aesthetically pleasing. Its convex gingival surface lies within the concavity of the alveolar ridge, mimicking the emergence profile of natural teeth. However, it requires modification of the alveolar ridge surface and has a longer restoration cycle. It is generally used in areas with high aesthetic demand, such as anterior teeth.

6. **Other Pontic Designs**
Other designs include E pontics (Enhancing esthetics), F pontics (Flat-Pontic), S pontics (Step-Pontic), etc. These designs share the characteristic of having a flat contact surface between the gingival surface and the mucosa, applying uniform pressure on the mucosa. Studies suggest that this can facilitate the migration of gingival cells over the pontic, forming a gingival contour on the buccal aspect.


P.12 E-bridges, F-bridges and S-bridges
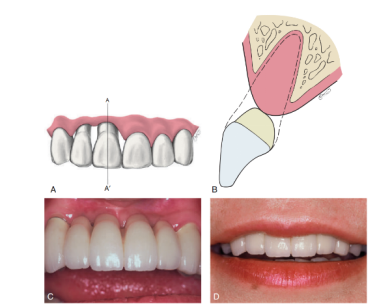
III. Design of the Axial Surface of the Pontic
1. **Convexity of the Labio-Buccal and Lingual-Palatal Surfaces**
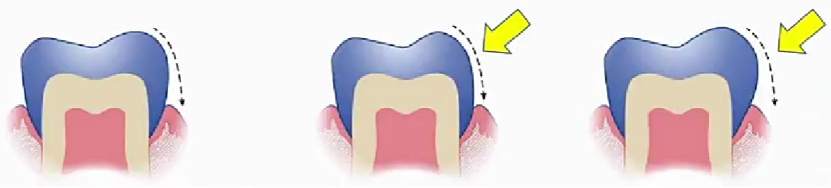
Similar to natural teeth, if the convexity of the axial surface of the pontic is inadequate, the gingiva will be subjected to excessive food impact; if it’s too pronounced, the gingiva will not receive physiological massage.
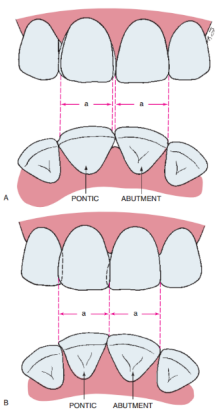
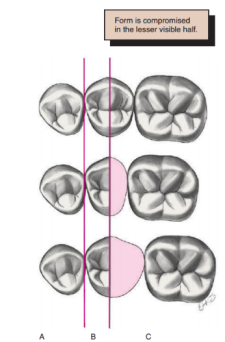
2. **Axial Surface Proportions**
The morphology of the axial surface of the pontic should closely resemble that of the contralateral tooth. If the edentulous space is too wide or narrow, adjustments to the axial proportions can create visual discrepancies to enhance aesthetics. For the anterior region, adjustments can be made by altering the morphology and line angles of the adjacent areas to compensate for space differences. In the posterior region, adjusting the proportions of the non-visible distal part of the axial surface can help reconcile space differences with the contralateral tooth. Additionally, methods such as adding extra developmental grooves on the buccal surface, adjusting the axial surface of adjacent teeth, and modifying the convexity of the buccal surface can be employed to address spatial discrepancies or create visual errors.
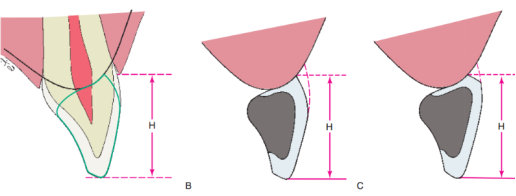
3. **Cervical Margin**
After tooth extraction, the alveolar bone undergoes resorption and remodeling. If the cervical margin of the pontic is designed to match that of the missing natural tooth, the pontic may appear overly long. Thus, the cervical third of the pontic should be slightly recessed, with the buccal third increased in convexity to improve aesthetics. When there is significant bone loss that hinders normal pontic coverage of the alveolar ridge, one approach is to simulate the exposed tooth root with part of the pontic, staining it to mimic exposed dentin; another method is to use pink porcelain to simulate gingival tissue, but this increases mucosal contact, making plaque control challenging.

4. **Interproximal Spaces**
The interproximal spaces on the lingual or palatal surfaces should be enlarged to facilitate food drainage and reduce occlusal forces.
References
1. Zhou Yongsheng. Oral Restoration (3rd Edition). Peking University Medical Press, 2020.
2. Korman RP. Enhancing esthetics with a fixed prosthesis utilizing an innovative pontic design and periodontal plastic surgery. J Esthet Restor Dent. 2015;27(1):13-28.
3. Gomez-Meda R, Esquivel J. The flat and step (F and S) pontics. Novel pontic designs for periodontally reconstructed sites. J Esthet Restor Dent. 2022;34(7):999-1004.
4. Gomez-Meda R, Esquivel J. Perio-prosthodontic pontic site management, part I: Pontic designs and their current applications. J Esthet Restor Dent. 2023;35(4):609-620.




Leave a Reply