
One of the reasons for the failure of root canal treatment is calcification within the canal path, which hinders reaching the proper working length completely. In some cases, dentists are unable to open calcified root canals and may suggest extraction. Therefore, once a calcified root canal is identified, clinicians should keep in mind the following basic principles of instrument operation proposed in this article.

Figure 1
A 38-year-old patient in good health visited my clinic, complaining of excessive sensitivity to cold stimuli in the right mandibular teeth. Tooth 46 was the most sensitive to cold stimuli (chlorothene). An initial periapical X-ray showed a large filling on the lingual wall of the tooth, a uniform high-density image (pulp stones) within the pulp chamber, and periapical lesions.
The formation of pulp stones may be related to long-term stimuli such as caries, deep fillings, and chronic inflammation. Some authors consider pulp stones as a manifestation of the pulp chamber trying to self-repair when stimulated (Goga et al., 2008).
Pulp pain caused by pulp stones is one of its common symptoms, ranging from mild to severe (Goga et al., 2008). Pulp stones may even lead to root canal blockage, resulting in the failure of root canal treatment.
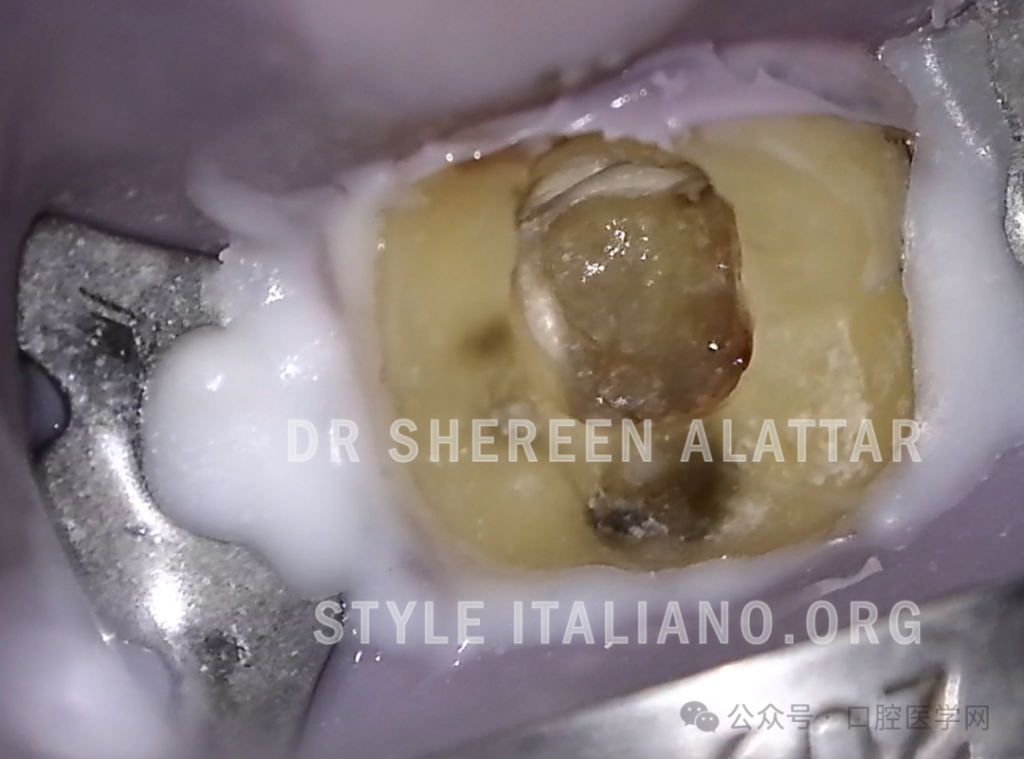
Figure 2
The preparation of the pulp chamber and removal of pulp stones were performed using an Acteon Satelec ET20 tip.

Figure 3
After removing the pulp stones filling the pulp chamber, three canal orifices were detected: the distal canal orifice, the mesial buccal canal orifice, and the mesial lingual canal orifice.

Figure 4
Without adequate vision and illumination to access the small canal entrance, clinicians may spend too much time searching for calcified canals, or may not be able to locate them at all. Worse, during this process, you are more likely to penetrate the tooth!
Furthermore, piezoelectric ultrasonic technology is highly effective in breaking through calcifications covering the canal orifice and in precisely removing valuable dentin while finding these canal orifices.

Figure 5
Once all calcified canals are identified, appropriate instruments should be used for clearance.
An unchanged basic principle of root canal instrumentation is “all root canal treatments should begin with small stainless steel hand files” (Patino et al., 2005). Therefore, I first used a pre-curved #8 K-file with a “watch-winding” motion to attempt to clear the distal canal and then switched to a #10 K-file upon reaching the full working length. Pre-bending and the “watch-winding” motion with hand files are crucial for handling calcified canals. Improper handling at this stage can easily create small steps or blockages at the apex, which will only worsen when using nickel-titanium rotary files. Additionally, apical patency may be easily lost in the process (Franco and Tosco, 2013).
Regardless of how small and flexible rotary files become on the market, they cannot replace initial stainless steel hand files in the early stages. Small hand files are vital for creating a “guide path.”
For both the buccal and lingual canals, I followed the same procedure, irrigating with sodium hypochlorite (at a 5.25% concentration) between instrument changes until the full working length was reached. At the apical area, I switched to a pull motion to make the file looser within the canal.

Figure 6
Subsequently, I used a thin nickel-titanium file with a tip diameter of 0.16 and a taper of 0.2, made of M-Wire, which provided some rigidity to ensure the safety of the canal path and remove restrictive dentine and other calcifications (Pullen, 2023).
In this situation of needing to clear narrow canals, following the manufacturer’s instructions, rotary files did not smoothly reach the expected working length. Therefore, I continued using the traditional method with the previously mentioned stainless steel K-files (#8 and #10) to complete clearance to the full working length.
Next, I proceeded with shaping files.
During the shaping process, always ensure the use of sodium hypochlorite irrigation to remove debris and recap and maintain apical patency after each shaping step.
Additionally, to enhance the disinfection of the canal system, I used an ultrasonic working tip to passively activate the sodium hypochlorite with ultrasound.
Figure 7
A fine medium gutta-percha cone was trimmed using a ruler, and the master cone fit X-ray was taken.

Figure 8
Root canal filling was performed using a hot gutta-percha vertical compaction technique, utilizing System B and Buchanan fine plugger with a temperature setting of 200°C.
Summary:
In conclusion, correctly handling calcified canals is crucial. Thanks to advanced magnification equipment and instrument technology, having the appropriate tools and following basic clinical protocols are extremely critical for managing calcified canals.
I also want to emphasize the importance of always considering your own capabilities. Even with the correct instruments and following the right procedures, you may find some calcified canals still challenging to handle. There is nothing wrong with stopping at the right time during the procedure. The key is knowing when to stop and refer. Overattempting to clear a canal without progress may worsen the situation by creating ledges or perforations.
References:
- Andreasen F.M., Kahler B. Pulpal Response after Acute Dental Injury in the Permanent Dentition: Clinical Implications—A Review. J. Endod. 2015;41:299–308.
- Oginni F.O., Kolawole K.A., Adekoya-Sofowora C.A. Evaluation of radiographs, clinical signs and symptoms associated with pulp canal obliteration: An aid to treatment decision. Dent. Traumatol. 2009;25:620–625.
- McCabe P.S., Dummer P.M.H. Pulp canal obliteration: An endodontic diagnosis and treatment challenge. Int. Endod. J. 2011;45:177–197.
- Goga R, Chandler NP, Oginni AO. Pulp stones: a review. International Endodontic Journal. 2008;41(6):457–468.
- Patiño PV, Biedma BM, Líebana CR, et al. The influence of a manual glide path on the separation rate of NiTi rotary instruments. J Endod. 2005;31:114-116.
- Franco V, Tosco E. The endodontic line: a clinical approach. G Ital Endod. 2013;27:2-12.
- Pullen R. Minimally invasive endodontics with a novel shaping file. Endodontic Practice US. 2023; 28:181-184.




Leave a Reply