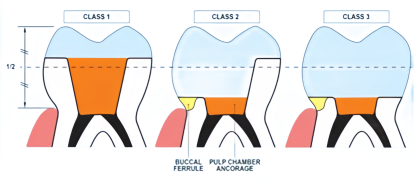
With the promotion of “minimally invasive” and “step-by-step” treatment concepts, along with advancements in restorative materials and adhesive technology, inlay-onlay crowns have gained popularity. These restorations provide a new option for post-endodontic coronal restoration by utilizing both mechanical retention from the pulp chamber and adhesive retention through a large contact area between the restoration and the tooth surface. Inlay-onlay crowns can be classified into three types:
Type 1: The tooth has at least two remaining walls, each with a height greater than half the crown height.
Type 2: The tooth has at least one remaining wall, with a height greater than half the crown height.
Type 3: All walls have a height less than half the crown height.
The preparation method may vary slightly depending on the type of defect.
Indications for Inlay-Onlay Crowns
Large Defects in Molars or Premolars:
Inlay-onlay crowns are suitable for restoring molars or premolars with extensive coronal defects. The tooth should have undergone thorough root canal treatment, exhibit healthy periodontal tissues, and withstand normal occlusal forces. The defect may range from three remaining tooth surfaces to no intact tooth walls. To provide sufficient retention, the remaining tooth structure should be supragingival, with continuous axial walls at least 1mm in height and 1mm in thickness.
Short Clinical Crown with Limited Retention:
Inlay-onlay crowns are particularly suitable for cases where the occlusal-gingival distance is short, preventing sufficient retention for a full crown, and where narrow, curved, or calcified root canals make post-core crown restoration inappropriate. For molars with short occlusal-gingival distances, axial wall reduction during full crown preparation can further reduce the remaining dentin support after endodontic treatment. Post-core crown restoration may not provide adequate retention height due to limited occlusal space, and periodontal crown lengthening might be necessary but costly and time-consuming. Inlay-onlay crowns can protect the tooth structure against vertical forces while reducing the need for multiple follow-up visits compared to other restoration options.
Contraindications:
Inlay-onlay crowns are not suitable when the remaining tooth structure is less than the above standards. If the defect is limited to an access cavity, a more conservative approach such as direct composite resin filling is recommended, making inlay-onlay crowns unnecessary. For cracked teeth or teeth under high functional stress (e.g., bruxism patients or abutment teeth), there is currently insufficient evidence supporting the reliability of inlay-onlay crowns; full crowns are recommended instead.
Management of Pulp Chamber and Canal Orifices
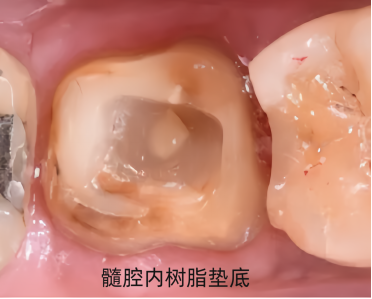
Proper sealing of canal orifices helps prevent reinfection, and the shape of the pulp chamber floor and cavity significantly influences stress distribution on the restoration. When preparing the canal orifice, the removal of gutta-percha should not exceed 2mm, and the integrity of the canal orifice pathway must be maintained without removing parts of the pulp floor, which should retain its saddle shape. If there are undercuts in the pulp wall, they can be filled with resin to maintain a rounded contour consistent with the original shape of the pulp chamber, promoting more even stress distribution.
Selection of Lining Materials
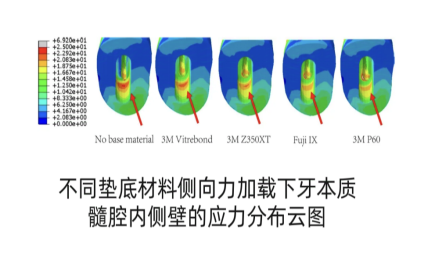
Materials such as glass ionomer cement, zinc phosphate cement, flowable resin, and composite resin are commonly used as lining materials in clinical practice. Recent studies indicate that as the elastic modulus of the lining material increases and approaches the elastic modulus of dentin, the peak stress on the remaining tooth structure decreases. Research by Yamamoto et al. found that with an increase in the elastic modulus of the lining material, the tensile stress on the tooth structure is reduced. Therefore, selecting a composite resin material with an elastic modulus closest to that of dentin is more beneficial for alleviating stress concentration on the tooth structure.
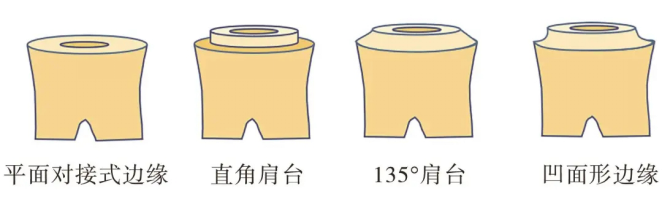
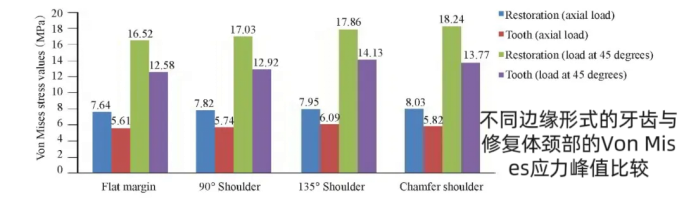
Design of Inlay-Onlay Crown Margins
The margins can be designed as butt joints, groove types, or wrap-around axial surfaces, depending on the clinical situation. Among them, curved and flat butt joints have similar stress distribution, with butt joint margins offering better protection for enamel and improving stress management in the restoration. Flat butt joint margins, right-angle shoulder margins, concave margins, and 135° shoulder margins show progressively increased stress at the cervical area. Studies indicate that with a bevel angle of 20°, the stress on dentin is reduced, making it more suitable for pulp chamber-retained crowns. Compared to other joint types, flat butt joints preserve more tooth structure and reduce cervical stress, making them preferable when there is minimal tooth structure loss.
Tooth Preparation
Occlusal Surface Preparation: Reduction of 1.5-2 mm using a wrap-around or butt joint margin. If the proximal surfaces are intact, mesial and distal margins can avoid the contact area.
Pulp Chamber Preparation: Removal of filling material in the pulp chamber and up to 2mm below the canal orifice, followed by resin sealing of the canal orifice.
Pulp Wall Shaping: Resin is used to fill undercuts in the pulp walls, creating an outward taper of approximately 5°-7°.

References:
[1]Gianfranco Politano,Bart Van Meerbeek Pemans.Nonretentive Bonded Ceramic Partial Crowns: Concept and Simplified Protocol for Long-lasting Dental Restorations.【J】Adhes Dent 2018;20:495-510.
[2]Stefano Bottachiari.Composite inlays and onlays复合树脂嵌体与高嵌体【M】周锐译.辽宁:辽宁科学技术出版社,2016-6.
[3] Tribst J P M, Dal Piva A M O, De Jager N,et al. Full-Crown Versus Endocrown Approach:A 3D-Analysis of Both Restorations and the Effect of Ferrule and Restoration Material(J].J Prosthodont, 2021,30(4): 335-344.
[4] 王剑. 浅谈嵌体和高嵌体修复的临床应用[J]. 国际口腔医学杂志, 2021, 48(5):9.
[5]程侠,张修银,吴艳玲,等.不同垫底材料对髓腔固位冠抗折性能影响的三维有限元分析[J].口腔颌面修复学杂志,2021,22:43-47+60.
[6]Ang Y, Tew | M. Conservative management of extensively damaged endodontically treated tooth using computer-aided design and computer-aided manufacturing-based hybridceramic endocrown: A clinical report[J]. J Conserv Dent, 2020,23(6):644-647.




Leave a Reply