Definition of Maxillary Sinus Septum
The maxillary sinus septum is a bony structure originating from the inferior or lateral wall of the maxillary sinus, which can divide the sinus cavity into two or more smaller cavities and is more commonly found at the base of the maxillary sinus.
The maxillary sinus septum is the main anatomical factor for the perforation of the mucoperiosteum during maxillary sinus floor elevation.
The BITC classifies the bony protrusions at the base of the maxillary sinus as “maxillary sinus septum” and “maxillary sinus minor septum”.

In 1910, Underwood described it as a structure of the cortical bone wall within the maxillary sinus, resembling an inverted Gothic arch, originating from the inferior or lateral wall of the maxillary sinus and capable of dividing the sinus cavity into two or more smaller cavities. In 1986, Tatum put forward the concept of maxillary sinus elevation, expanding the indications for posterior tooth implantation in the maxillary region. In 2012, Ogle et al. defined it as a bony pillar within the maxillary sinus with a height of at least 2.5 mm.
So, is there a difference in the occurrence probability of the maxillary sinus septum among different populations? From domestic and foreign studies, we have concluded that the maxillary sinus septum is a common anatomical structural variation, and its occurrence probability has no difference with gender or age.
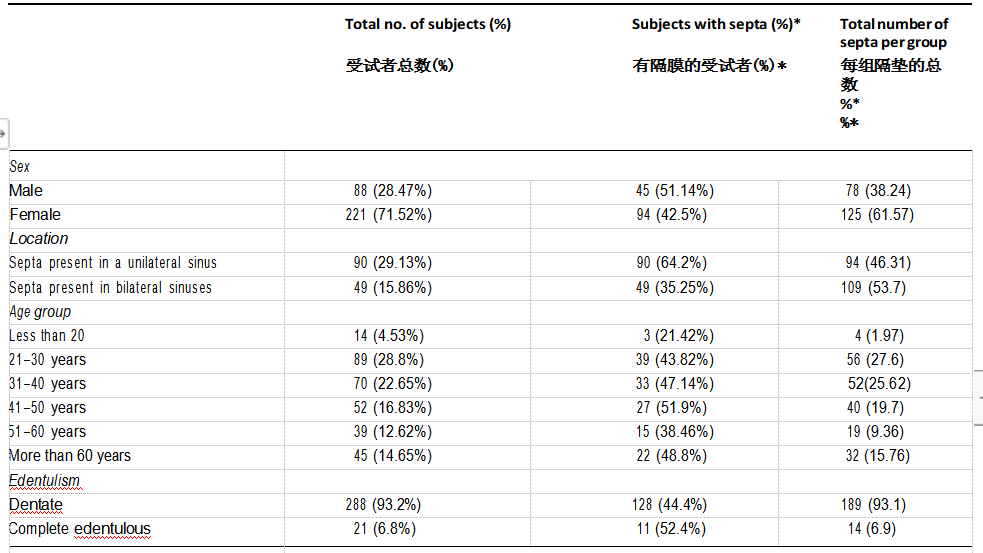
According to the conclusion drawn from this literature: When divided by gender and age, the prevalence of the maxillary sinus septum among the included subjects has no statistical significance (p = 0.32 and p = 0.09 respectively).
Causes of the Formation of Maxillary Sinus Septum
The maxillary sinus septum is divided into primary septum and secondary septum.
The primary septum is a congenital developmental septum, and its formation mechanism is not yet clear. It may originate during the development of the maxillary sinus and the eruption of teeth. Some septa are relatively large and can even extend from the base of the maxillary sinus to the superior wall.
The secondary septum is an acquired septum and may be the result of maxillary sinus pneumatization. The pneumatization of the maxillary sinus (especially the pneumatization at the base of the sinus) is uneven, forming bone ridges protruding into the sinus, usually small septa at the base of the sinus. The resorption of the alveolar ridge caused by tooth extraction, pathology or trauma also increases the occurrence of septa.
Classification of Maxillary Sinus Septum
Type I Septum
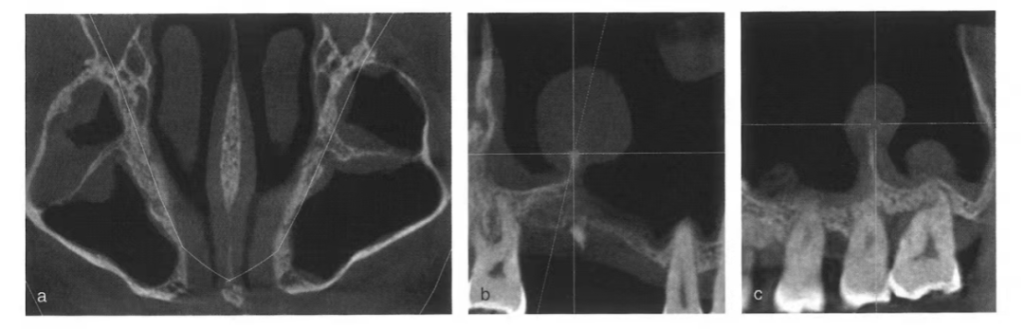
CBCT scans of a middle-aged male, showing the horizontal plane (a) with the vertex of the sinus floor septum (the intersection of the crosshairs) as the region of interest, and the mesiodistal sections of the right (b) and left (c) sides in sequence. The bilateral sinus floor septa run in the buccolingual direction, dividing the sinus floor into anterior and posterior parts. There is varying degrees of mucoperiosteal thickening before and after the septum, and there are also pseudocysts. The horizontal plane section is crucial.
Type II Septum

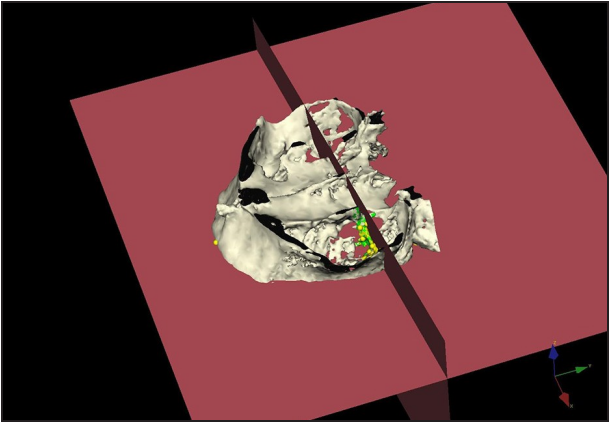
CBCT scans of a young female, showing the coronal plane (a), sagittal plane (b) and horizontal plane (c) sections with the septum (the intersection of the crosshairs) as the region of interest, and the horizontal plane section at the upper part of the septum (d) in sequence. The septum runs in the anteroposterior direction and reaches the superior wall of the sinus cavity. It has no contact with the lateral wall at the sinus floor, forming two compartments inside and outside, sharing the same maxillary sinus opening. The sagittal plane section is crucial.
Type III Septum

CBCT scans of a young female, showing the coronal plane (a), sagittal plane (b) and horizontal plane (c) sections with the septum (the intersection of the crosshairs) as the region of interest. The horizontally running septum divides the maxillary sinus into upper and lower parts, sharing the same maxillary sinus opening. The sagittal plane section is crucial.
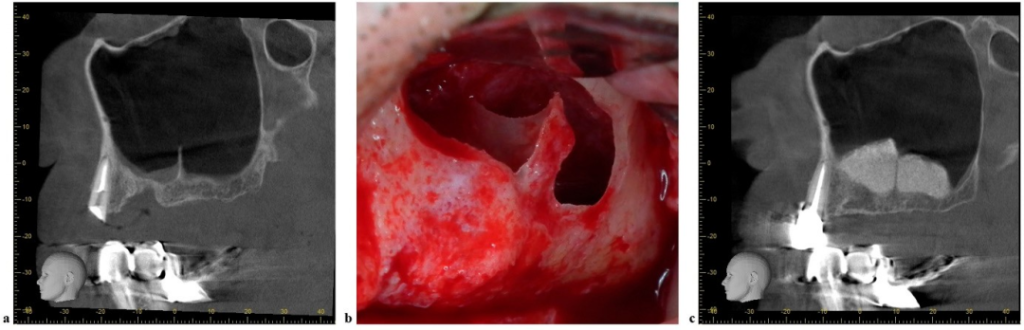
Type IV Septum
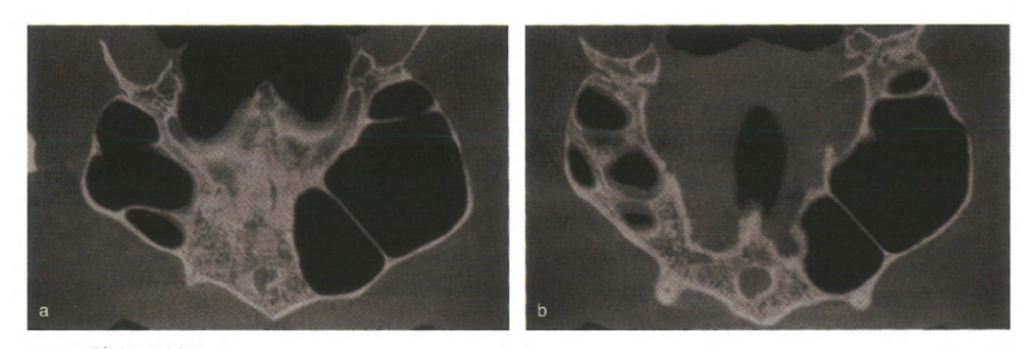
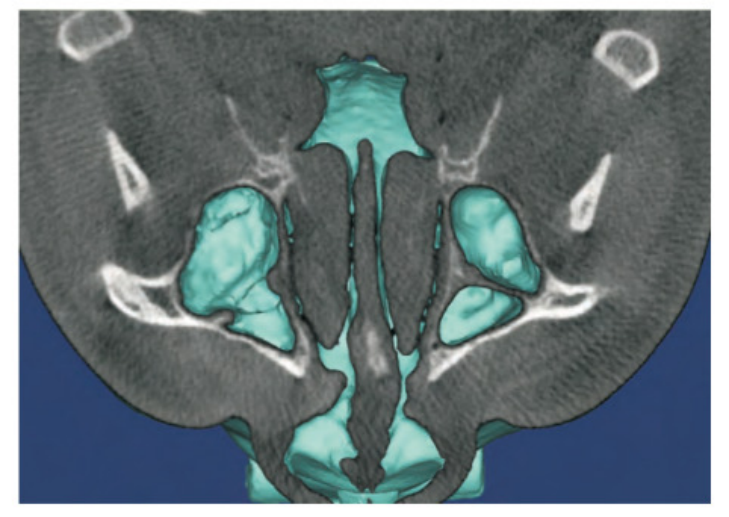
Horizontal plane sections of the hard palate (a) and below the hard palate (b). The bilateral maxillary sinuses are extremely asymmetrical, with the right side being significantly smaller than the left side. The left sinus cavity expands anteriorly approaching the midline. There are mixed-type septa in the bilateral sinus cavities. The right sinus floor is divided into four parts by septa running in the buccolingual and horizontal directions.
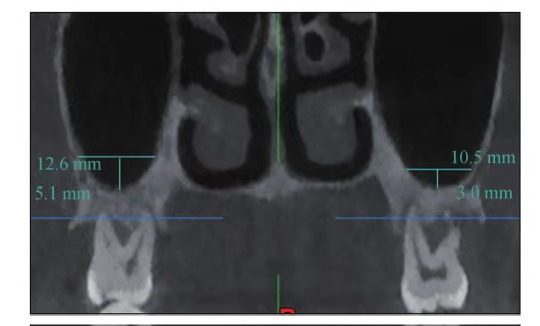
Definition of the Buccopalatal Width of the Maxillary Sinus Cavity (BPSW) and the Maxillary Sinus Angle
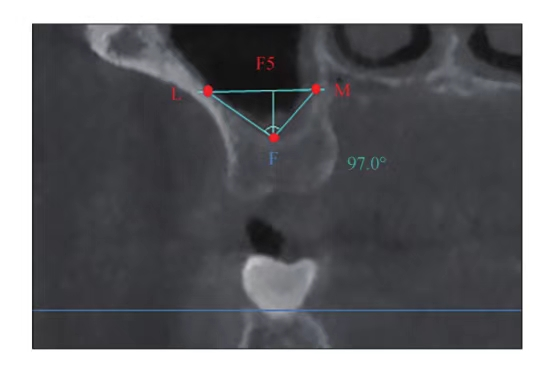
A retrospective study found that the average value of MSA is 95.5°. When MSA < 90°, the incidence of maxillary sinus membrane perforation is the highest (38%), almost twice that when the angle > 90°.
A 2020 study analyzing the factors influencing bone formation in maxillary sinus floor elevation via the crestal approach showed that MSA was 78.09° ± 10.27°, and there was a positive correlation between MSA and the bone resorption at the implant root end, indicating that the larger the angle between the buccal and palatal bone walls of the maxillary sinus, the more the absorption of the bone graft material.
When the maxillary sinus membrane is elevated to the same extent, the tension of the wider maxillary sinus membrane is greater than that of the narrow membrane, and the increased tension of the maxillary sinus membrane is directly transmitted to the graft material or blood clot, resulting in more bone resorption.

From this expert consensus, we can understand the impact of the existence of the maxillary sinus septum on bone formation.
The existence of the maxillary sinus septum will increase the difficulty of maxillary sinus floor elevation. The maxillary sinus septum itself has no obvious impact on the formation of inflammation. Improper operation causing damage or perforation of the maxillary sinus mucoperiosteum will lead to the occurrence of maxillary sinusitis and affect bone formation.
Avoid performing transalveolar maxillary sinus floor elevation at the bone ridge to prevent the sharp bone ridge from puncturing the mucoperiosteum at the base of the maxillary sinus and causing perforation of the maxillary sinus floor, resulting in maxillary sinusitis and affecting bone formation.
Meanwhile, there are also studies attempting to use the maxillary sinus septum as an alternative source of available bone height to treat patients with missing teeth. The average increased bone height in the experiment was (2.18 ± 1.47) mm, so that longer implants can be implanted. Implants with a diameter of 4 mm and a height of 7 mm fit the maxillary sinus septum best. It can also better adjust the axial angle of implant placement (45° – 135°).
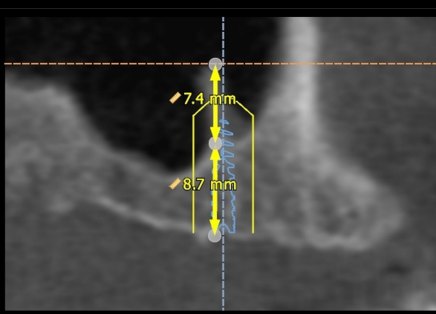
As shown in the figure: Measure the height of the crest and the septum on the two-dimensional reconstructed image.
Treatment Methods and Principles for Maxillary Sinus Septum
Selection of the Location for Window Opening
When the septum has no contact with the lateral bone plate of the maxillary sinus and the internal and external movement of the bone plate after window opening will not be affected, the maxillary sinus membrane can be normally dissected after opening a window on the lateral wall of the maxillary sinus. If the septum does not contact the lateral bone plate of the maxillary sinus but is within the dissection range of the maxillary sinus mucoperiosteum, a bone window can also be opened on the lateral wall of the maxillary sinus.
Multiple Bone Windows When the septum has complete or incomplete contact with the lateral bone plate of the maxillary sinus, windows can be opened on both sides (mesial and distal sides or above and below) of the maxillary sinus septum to avoid it, and the sinus membranes attached to the base of the maxillary sinus and on both sides of the septum in the two bone windows can be dissected respectively. After elevating them, bone augmentation materials can be implanted simultaneously.
How to Treat the Septum and Dissect the Maxillary Sinus Membrane?
① Dissect the maxillary sinus floor and the sinus membrane attached to the bone surface of the septum. After complete exposure, implant bone augmentation materials directly without treating the septum.
② Dissect the maxillary sinus floor and the sinus membrane at the base of the septum at the sinus floor, then cut off the base of the septum. Pay attention not to cause unnecessary fractures and mucoperiosteal damage. After complete disconnection, peel off and lift the septum together with the sinus membrane, or place the bone augmentation material after removing the partition.
Principles and Methods for Treating the Septum in Transalveolar Maxillary Sinus Floor Elevation
If the site of maxillary sinus floor elevation does not involve the septum, conventional transalveolar maxillary sinus floor elevation can be carried out.
If the site of maxillary sinus floor elevation involves the septum, including when the septum is located above the site of maxillary sinus floor elevation or within the range of maxillary sinus floor elevation, it is not recommended to carry out conventional transalveolar maxillary sinus floor elevation, and it should be changed to lateral wall window maxillary sinus floor elevation.
references
[1]Three-Dimensional Evaluation of Implant Positioning in the MaxillarySinus Septum: A Retrospective Study2015
[2]宿玉成,上颌窦底提升2022
[3]中华口腔医学会口腔种植专业委员会.上颌窦底提升专家共识:上颌窦间隔[J].中国口腔种植学杂志,2024,29(2) 103-108.DOI:10.12337/zgkqzzxzz.2024.04.003.
[4] Cheng XH, HuXC, Wan SQ, et al. Influence of la-
teral-medial sinus width on no-grafting inlay osteo- tome sinus augmentation outcomes[J]. J Oral Maxil- lofac Surg, 2017, 75(8): 1644-1655.
[5] 何添荣,陈玉英,许香娜,等.上颌窦内外侧宽度对
不植骨上颌窦内提升的成骨影响[J].口腔生物医学,2021,12(4): 257-261.
He TR, Chen YY, Xu XN, et al. Influence of lateral- medial sinus width on the outcomes of sinus eleva- tion without graft via transcrestal approach[J]. Oral Biomed, 2021, 12(4): 257-261.
[6] 范震,王方,王佐林.经牙槽嵴顶上颌窦底提升术:
中华口腔医学会第五届口腔种植专业委员会学术共识[J].口腔颌面外科杂志,2018,28(1):1-9.
Fan Z, Wang F, Wang ZL. Academic consensus reached in the 5th oral implant committee of Chi- nese stomatological association-the crestal approach sinus augmentation[J]. J Oral Maxillofac Surg,2018,28(1):1-9.
[7] 肖剑锐,李德华,马威,等.上颌窦提升后植骨区垂
直高度的变化及分析[J].口腔医学研究,2008,24(2):209-211.
Xiao JR, Li DH, Ma W, et al. Analysis of the trans- planted bone level after maxillary sinus elevation[J]. J Oral Sci Res, 2008,24(2):209-211.
[8] Pizzini A, Basma HS, Li P, et al. The impact of ana-
tomic, patient and surgical factors on membrane per- foration during lateral wall sinus floor elevation[J]. Clin Oral Implants Res, 2021, 32(3): 274-284.




Leave a Reply